

Living with a chronic liver condition is not merely an issue for doctors; it’s a continuous fight. The fatigue, swelling, and hospital visits that appear to be on the same schedule. For many patients, conventional treatments will eventually prove insufficient. This is what no one can prepare patients for.
Indeed, the DIPS process isn’t talked about in the way it ought to. However, for patients who have exhausted all other options, it’s been gaining recognition as one of the most crucial instruments in the field of modern interventional medicine.
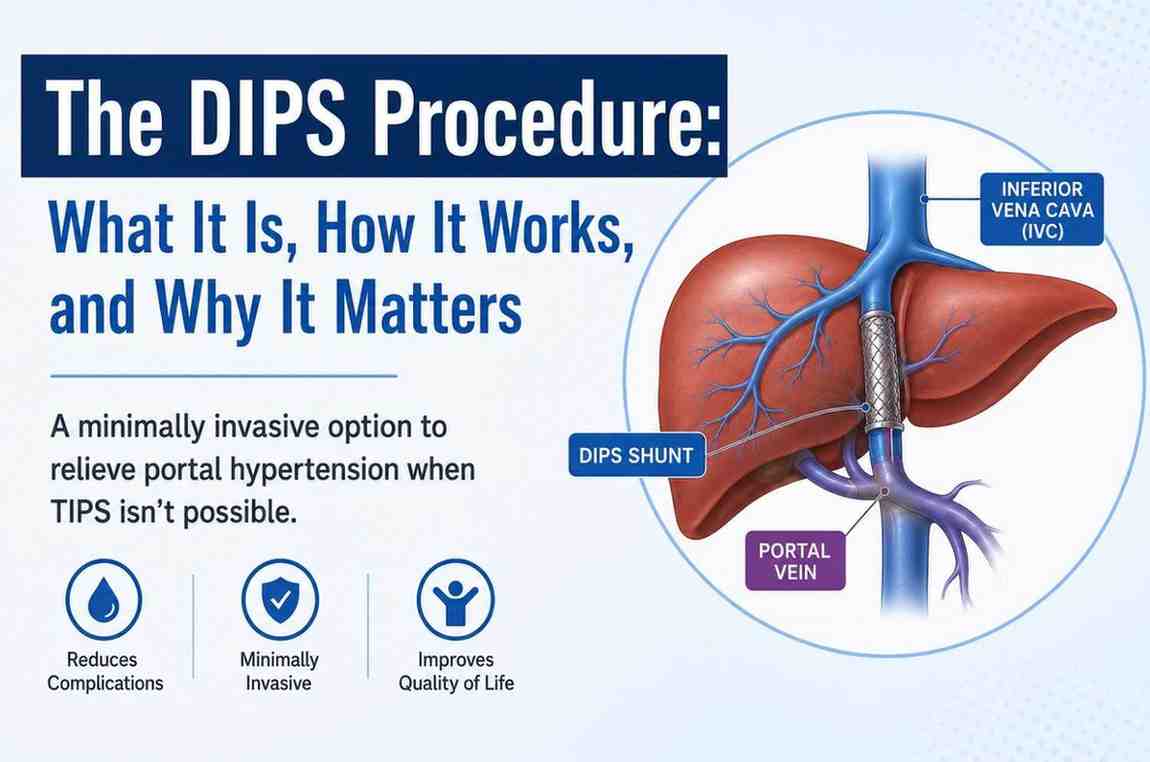
DIPS is a shorthand for Direct Intrahepatic Portocaval Shunt. It sounds complicated; however, the concept is easy when you understand it.
The portal vein is the conduit for blood from your intestines, stomach, and spleen to the liver. If the liver’s disease- which is most often cirrhosis- results in the liver becoming scarred, the flow of blood to the liver becomes limited. Pressure builds up in the portal vein. The body attempts to redirect the flow of blood to smaller vessels, which were not designed to carry this kind of burden.
This is where things can get very dangerous.
Smaller vessels, such as those in the stomach and esophagus, could swell up and break. In the abdomen, fluid accumulates. Toxins that should be removed by the liver are able to enter the brain. The entire chain of events can be classified as portal hypertension and is the primary issue that the DIPS procedure was created to solve.
It creates an immediate conduit (called a Shunt) connecting the portal vein with the hepatic artery inside the liver. This provides blood with a brand new pathway that is of lower resistance and alleviates the pressure on the vessels that are brittle and overloaded.
The majority of people are familiar with TIPS – Transjugular intrahepatic Portosystemic Shunt. TIPS has been in use for many years and is based on the same fundamental concept: to create a shunt in order to alleviate pressure on the portal.
The difference lies in how you go about getting there.
TIPS is done by inserting a jugular vein catheter in the neck, guiding catheters downwards toward the liver. For most patients, this is a good option. However, anatomy can be a challenge. Certain patients have vascular problems which make the jugular route difficult or even impossible. Some have had a prior TIPS shunt which stopped working or became blocked.
DIPS follows a more direct route right through the skin to the liver. There is no need for jugular access. It’s a more technical method; however, it allows patients who otherwise would have few alternatives.
The eligibility of DIPS is determined on a case-by-case basis; however, there are a variety of situations where it is the best option for you.
Patients suffering from portal hypertension due to cirrhosis who suffer from bleeding from varices in the esophagus, regardless of medications or endoscopic treatments, are usually the best candidates. Also, patients suffering from chronic ascites, which is a type of persistent abdominal fluid accumulation that doesn’t stop recurring regardless of how often it’s flushed or how rigorously diuretics are prescribed.
Budd-Chiari’s Syndrome, a rarer condition that causes blockage of the liver’s hepatic veins and intestines, is another scenario in which DIPS is particularly effective. Patients with a malfunctioning or failed TIPS shunt frequently discover that DIPS is an effective corrective option in cases where reversing the jugular route doesn’t work.
The process of evaluation involves thorough imaging, such as CT scans, MRIs, and Doppler ultrasounds, to determine precisely what’s happening within the liver’s vascular system before any procedure is planned.
In the context of such important results, the DIPS procedure is actually not very invasive from a surgical point of view. There’s not a large cut. No open surgery. The majority of patients are sedated instead of full general anesthesia.
The interventional radiologists use a needle to enter the liver through the skin. The procedure is supported by real-time ultrasound or fluoroscopic imaging. Once inside, catheters and wires are utilized to traverse the portal vein and form the channel known as the shunt. A small-sized stent is inserted to keep the vein open and ensure the flow of blood.
The pressure inside the portal vein is assessed prior to and after the procedure to ensure the procedure was successful. The entire procedure typically lasts between 1 and 3 hours. Most patients spend one or two days under observation before going back home.
Take a look at the time it takes to recover compared with open surgical options, and you’ll begin to comprehend why minimally-invasive procedures such as this are now the standard of care in areas where they’re offered.
The most frequent thing that patients mention in the weeks after DIPS is a significant change in their body. A decrease in gastric discomfort. Fewer bleeding episodes. More energy. The chronic background pain that is associated with portal hypertension begins to subside.
It is essential to follow up regularlyIt is important to follow-up regularly. Doppler ultrasounds are generally scheduled to verify that the shunt is still functional and open. The changes in diet, especially cutting down sodium and staying clear of alcohol, will remain an important aspect of the long-term plan. For patients who are waiting for the possibility of a liver transplant, DIPS may serve as an important bridge to stabilize their situation until a donor is found.
It’s important to clarify: DIPS doesn’t reverse liver disease. It is able to manage the negative effects that it has, and in a lot of instances, it handles them well.
This isn’t a process that can be carried out anyplace. The technical complexity requires the expertise of a group with experience in both interventional radiology and the field of hepatology. Before proceeding, inquire about the number of cases, outcomes data, and what the follow-up procedure will look like.
The most effective centers view DIPS not as a stand-alone intervention, but as a component of a comprehensive treatment plan that is based on the patient’s particular conditions, goals, as well as general health condition.
For those who have been told they’re not getting any alternatives and are told they’re out of options, the DIPS procedure is a real thing and not a miracle or a breakthrough, but an important move forward. It’s a type of treatment that meets patients at their current location and offers them more time, greater stability, and, in many instances, an improved quality of life.
If portal hypertension, or any of its complications, is a part of your experience, this is a discussion to have with a doctor who has a good understanding of this field.
© 2025 Crivva - Hosted by Airy Hosting Managed Website Hosting.








